- 5 Simple Tips For Breastfeeding A Small Baby - February 5, 2026
- Supporting Immigrant Families Through Birth: 5 Organizations To Support - January 29, 2026
- Podcast: How Emotional Support Can Change Lives In Childbirth with Founder Suzzie Vehrs - January 23, 2026
Hey there mama, you are here because you have decided that you are team epidural, and you are a bit nervous about tearing during labor. Is it possible to deliver a baby without tearing while using an epidural? And, what is that laboring down thing that is becoming more and more popular? How and why does this method of pushing make a difference?
If you are like most moms, you have heard stories of moms tearing while pushing, of moms pushing for hours, and of moms going back for surgical births while they were pushing. You would like to avoid these outcomes if possible. On top of that, you are proactively setting up your birth plan to set you up for success!
But, you also have heard mixed things about laboring down and wonder if it will work for you? or if it is the safest way to go?
Well, welcome to our guide on laboring down where we will explore the pros, cons, alternatives and logic behind this strategy.
We will start by talking about the risk of tearing, what it is, how common it is, and some best practices for reducing the risk!
After you’ve read this post, I hope you have the information you need to make a centered decision about your desired strategy for the pushing phase of your epidural birth!
More than that, I hope that whatever you decide is your preference, laboring down or not, you gain confidence in your own voice and your ability to advocate for yourself during labor. Let’s get started!
How Common Is Tearing In Labor?
Tearing is understandably a part of labor many women are concerned about. There are quite a few reasons we want to avoid larger tears:
Perineal tears affect about 80% of women during childbirth, with first time moms being affected more frequently than moms giving birth for a second time or more. [1, 2].
But, tears are not all the same. Some are much more more difficult to heal from than others. So what are the different types of tears?
1st degree tears:
1st degree tears are quick easy and easy to heal from. It is a small tear of only skin and vaginal mucus. You might think of this as a skidmark, or papercut. It is small, not terribly painful and will heal nicely.
2nd degree tears:
2nd degree tears are a bit deeper. They involve a bit of muscle tearing, but, the muscle of the sphincter is not involved at all. Usually a 2nd degree tear will require just a couple stitches, placed with local anesthesia to make sure it heals properly.
3rd degree tears:
3rd degree tears are the type of tears that may require more intense care and time to heal. I believe all moms deserve to see a pelvic floor physical therapist after giving birth, but if a mom has a third degree tear or more, it becomes even more important. A 3rd degree tear goes deeper into the muscle, going far enough to involve the anal sphincter complex.
4th degree tears:
4th degree tears are both quite rare and quite worrisome. These extend to the epithelium or rectum. Moms with fourth degree tears will usually need to go to the operating room for a more involved repair.
Why We Need To Take Steps To Limit Tearing During Childbirth
Tearing during childbirth may seem inevitable to some. Many believe it is ‘just part of the process’. But, I think we need to be careful accepting that as a norm we have no control over – because we can actively support pushing and limit tearing. Tearing can lead to long term physical, psychological and social problems.
While moms with lesser tears will likely feel better within 2-8 weeks, moms with larger tears may still have pain 18 months later. Perineal pain can affect breastfeeding when it makes it impossible for a mother to get comfortable. And, like any chronic pain, can affect a mothers mood.
For those 3rd and 4th degree tears, anal and urinary incontinence can last long after birth. Pelvic organ prolapse and difficulty enjoying sex can be ongoing difficulties.
It is crucially important for all mothers that health care teams are actively seeking to reduce tearing. And we are just about to discuss one strategy that I’ve seen work many times.
How Common Is It To Tear During Labor?
The good news is that 3rd and 4th degree tears remain relatively rare.
The most common type of tear in the US right now is a second degree tear.
For first time moms 2nd degree tears are reported to be between 35-78% of births where a mom is having her first baby and 35-40% of second time moms. [1–3]. Third- and fourth-degree tears, which involve varying degrees of injury to the anal sphincters, occur in 5.1–8.3% of first time moms and 2-3% of moms having a second (or more) baby.
Is It Possible To Have Fewer Tears?
But, just because tears are extraordinarily common – doesn’t mean that they HAVE to be that common.
Some providers have MUCH different results.
For example, for one group of midwives more than half of women (58.3%) of mothers had NO TEARS while delivering their babies. Another 41.5% of moms had first degree tears only. Less than 1% had a second degree tear.
And the news gets even better, when it comes to the larger tears that have potential long term impacts, out of nearly 2,000 women, only 1 woman had a 3rd degree tear, and no one had a fourth degree tear.
Clearly we can learn to manage the pushing phase of labor with less intervention + less damage to mothers.
In the study published on the midwives mentioned above, it was very clear that they have an overarching belief behind the support they give in the pushing part of labor. They do not support prolonged bearing down efforts.
But how can we bring that strategy of less pushing into the hospital where more intervention is common? Is it possible for a woman without an epidural to limit how long she actively bears down? I don’t want to spoil the answer, but it is a resounding yes!
What Is Laboring Down?
Laboring down is a strategy of pushing. The goal of this strategy is to support the work a mother’s body is already doing, by not interfering with immediate, directed pushing when a mother reaches 10 cm dilated. When laboring down, a mom puts more trust in her body, and waits to push.
This is an effective way to limit the amount of time that she has to actively push or bear down.
During this time, she trusts her body will continue to move her baby down, and that the baby will continue to work through their cardinal movements and rotate to align the smallest part of their head with the the exit!
She does that to reduce potential trauma to her baby and her body in the delivery process.
Jessica’s Laboring Down Story
Jessica was a mother I worked with when I first discovered the strategy of laboring down. Though she dreamt of a home birth, she had pre eclampsia and needed to do an induction in the hospital. We had talked about laboring down as an option to reduce trauma to her body. And she ran with the idea.
In her inductions, as she began to feel pressure in her pelvis, she pressed the little epidural button that gave her more pain relief. She had some flavored ice chips (from a slushy machine she had brought herself!) and we waited. She let her nurse know that she wasn’t quite ready for a check or to push, though she thought she was close because she felt pressure and almost like she had to poop.
These are two pretty reliable signs a mother with an epidural is either close to 10 cms or there already!
Even with these signs, we waited and waited.
Eventually, she told me she felt like there was something coming out of her.
I ran to get her nurse – who ran to get her doctor. Jessica was right – her bag of waters WAS just starting to come out of her.
As her doctor came into the room, her baby crowned and her doctor caught the baby before he was even gowned up!
Jessica became the first woman with an epidural I ever worked with that had ZERO tearing. Since then, I have seen this repeated many times over.
Is Laboring Down Safe?
In 2008 a meta analysis of moms who choose passive descent, (another term for laboring down where 2 hours are provided after complete dilation before a mom pushes) vs immediate pushing was published. They found that
- passive descent increases a woman’s chance of having a spontaneous vaginal birth
- decreases risk of having an instrument-assisted deliveries
- decreases pushing time
The research concludes that allowing the fetus to passively descend the birth canal, instead of pushing immediately upon full dilation, is a safe and effective method of increasing spontaneous vaginal births, decreasing instrumental deliveries, and shortening pushing time.
How Long Do Mothers Typically Push If They Successfully Labor Down With This Definition?
Studies show that timing of pushing with an epidural is consistent in that delayed pushing leads to a shortening of the actual time pushing and an increase in spontaneous vaginal delivery at the expense of an overall longer duration of the second stage of labour.
You spend more time waiting, but much less time pushing.
In my experience, moms who labor down often push for a surprisingly short time, or almost not at all.
After laboring down, prepare to push for a grand total of 15 minutes or less if you labor down to the point you can see your baby’s head at the vaginal opening. Yes, for most moms, laboring down means your baby almost births themselves.
Is it possible?
Yes! As a doula that has attended hundreds of births, I have seen this happen over and over again. In the last birth I attended before writing this, the mother pushed for a grand total of 9 minutes. The induction I attended before that? Even less.
You can see, there is a pattern here. My expectation is that if we delay pushing – a mom with an epidural rarely has to push for more than a few minutes.
This is much different than the regular expectation of 2-4 hours pushing for a first time mom with an epidural – which is expected if she begins pushing as soon as she reaches 10 cm dilated.
Where Did You Discover This Strategy?
I first learned this method from Dr. Rachel Reed, who has spent her career supporting physiological birth. She has an amazing book Reclaiming Childbirth as a Rite of Passage: Weaving ancient wisdom with modern knowledge, which I highly recommend if you are the type of person that likes to curl up with a good book + are seeking a more empowered birth experience.
How I Became Interested In Laboring Down
Hi, if we don’t know each other yet, my name is Suzzie. I am a doula and childbirth educator. And my goal is to help you create a birth that you love. Laboring down was not always a practice that I supported or even knew about.
Here’s my story.
The year was 2022, I had been a doula for nearly 3 years and I was frustrated.
As a doula, it was my job to help my clients navigate their birth, support them emotionally and physically and protect their right of informed consent.
One of the reasons I became a doula was because of the difference between my first and second birth – you can listen to my own birth stories here. I had an unexpected surgical birth with my first baby and a very empowering VBAC with my second.
Helping mothers prevent surgical births became somewhat of a passion of mine since then.
I also knew that the presence of a doula reduces the odds of cesarean delivery and instrumental vaginal delivery when compared with women receiving standard maternity care.
But I wasn’t always seeing that with my clients! I was frustrated at how often I was ending up in the OR, how many larger tears I was seeing, and the times when episiotomies (cuts into the vaginal wall) actually seemed needed was heart breaking. I felt like I was letting my clients down.
Why Were My Clients Having Surgical Births?
When I looked through every c-section I had in the year of 2020-2022, the most common surgical birth story was this:
Mom started labor, often with an induction, labor was long, we eventually made it through to pushing, sometime during the pushing phase of labor, baby would crash, or more frequently, wouldn’t move fast enough and the mom was told the baby ‘didn’t fit.’
After 2, 3 or 4 hours, with different cutoffs provided by different providers, the doctor or midwife would say ‘you haven’t made enough progress, it’s time for surgery.’
Looking at my own data led me to the realization that something needed to change in the way I supported and guided moms in the pushing phase of labor – particularly for moms with epidurals.
Because that’s when moms were going to surgery. As a mom who has never regretted my own choice to meet my pain management needs with an epidural in my first labor, I was a bit heartbroken by this and wanted to do better by these moms.
Where Was The Problem?
I already knew that directed pushing, pushing where an outside person, myself or a nurse, midwife or OB, would tell a mom how and when to push while encouraging her to hold her breath, could cause problems with the pushing part of labor for a mom without an epidural.
But I also knew that it was really difficult for a mom with an epidural to direct her own pushing phase. It doesn’t come as naturally when you’re numb.
Pushing can also be a lot of hard work, especially if done for hours. Many moms battle fatigue and have to dig deep during the pushing phase of labor – at least, that is what was the normal for my moms before we switched to laboring down.
How Does Directed Pushing Impact The Labor Process?
How can directed pushing, or an outside person telling you to push for 10 seconds at a time, multiple times through a contraction, lead to problems?
Directed Pushing over a period of time can lead to problems like these for a mother:
- When you hold your breath to push, it can change the PH levels in your body. The PH change leads to your uterus having less strong contractions. Weaker contractions are less effective at helping a baby move down and out of the body. Your uterus is the largest and strongest muscle in your body at the time you give birth. But, if it’s not working as hard, you are going to have to push harder to make up the difference.
- All this extra work, telling moms to push harder and harder can then lead to maternal fatigue. Why? because now all that extra power has to come from self created power. As she pushes harder, she is using more and more energy and is more likely to reach exhaustion. Also, to get more output with each push, she is told to hold her breath longer, the Ph continues to change and the problem of step one is exacerbated. A cycle is created.
- This all leads to Increased risk of large tears + episiotomy use. Yes, directed pushing in moms without epidurals, leads to greater tears and more babies in crises. The true is same for moms with epidurals. And honestly, a baby in danger, whose heart rate is going down while a mom pushes, and is not recovering well when she takes a break, may need to be rescued with an episiotomy and forceps.
Let’s See This In Action With Ashley’s Birth Story
Real quick, I’d like to share Ashly’s birth story with you. She was a mom I was with who did have an episiotomy and 3rd degree tear. As she was pushing, her baby’s heart rate was going down, and taking it’s time to recover. With each push, the heart rate was going further down, and taking longer to come back up.
As is somewhat normal, the lower the baby moved in her pelvis, the more difficult it was for the nurse to keep the baby’s heartrate on the monitor. This is important because the heart rate is how we know if the baby is okay or not.
At one point in time, we saw the baby’s heart rate go down -concerningly far. As the heart rate reached it’s lowest point yet, the nurse lost the tracing on the monitor and could not find the baby’s heartbeat. We truly did not know if the baby’s heart rate had disappeared because something happened to the baby or if the baby was just in a really difficult position to find (which often happens right before they are born.) The doctor quickly suggested an episiotomy (a cut into the vaginal wall) and pulled the baby out with forceps.
I don’t think I’ve ever seen someone move so quickly.
Turns out the baby was quite healthy and just fine. We all cried tears of joy, because it was such an intense and scary moment. This lack of information, and potential for a life threatening situation led to quick and appropriate, but quite invasive action. Could the directed pushing that we had been giving Ashly have contributed to her baby’s distress in the first place?
The answer is yes.
How Directed Pushing Can Impact Babies Heart Rate + Oxygen Supply

One way directed pushing impacts babies is that it limits their oxygen intake. Moms hold their breath while they push to create enough power. Typically moms are directed to hold their breath for 10 seconds at a time and push. Getting 3 -5 strong pushes in with each contraction. However, over time, this can lead to less oxygen to the baby causing increased risks of hypoxia, or a dipping heart rate like Ashley’s baby had.
It is my experience that waiting until a mom does not need directed pushing, or only needs it for a short time, is good for both moms and babies.
For moms, it is simple less work to wait and let her body do the work of moving her baby down. For babies, they get more oxygen, because MOMS are getting more oxygen.
How Directed Pushing Can Affect Babies Pt 2
When a mom is forced to push and directed from the beginning, her baby can run into another challenge as well. Babies have a job to complete as they come into the pelvic outlet. They are completing what is called their cardinal movements. This is how they align with the best way to exit their mother’s body.
Some research shows that directed pushing can interfere with the gradual descent and rotation of the baby. It is a devastating thing to realize that the thing you were doing to help a baby be born, and is standard care, is actually making the process more difficult for them.
One of the most common reasons my clients were told their baby wasn’t making progress back in 2022 and before? Their baby was in a weird position. They weren’t moving. They didn’t ‘fit’.
After learning how directed pushing prevents babies from rotating and aligning, this makes a lot more sense. By pushing forcibly and immediately, we never allowed the baby time to complete their internal rotation before putting inappropriate amounts of pressure on them from our directed pushing. Essentially, WE WERE CAUSING BABIES TO GET STUCK.
Can Laboring Down Reduce C-Sections In The Pushing Phase Of Labor? Alex’s Story
Alex is a mom I worked with when I was in the process of investigating, gathering information and learning about laboring down. I was aware of it, but not confident enough to really promote it. Alex reached 10 cm and we were told by her OB to start pushing. Which we did. Time passed. Alex worked really hard and had pushed so much that she was reaching a place beyond fatigue. She was exhausted – and her baby had not moved one bit.
Alex’s Story Takes A Turn For The Worse: The Cephalopelvic disproportion (CPD) Diagnosis – Baby Is The Wrong Size And Doesn’t Fit
It was determined by the OB that the baby was in a ‘bad position’ and at 2 hours we were told there wasn’t enough progress made and time was up. It was time to have a surgical birth. If she hadn’t made any progress in 2 hours, the baby clearly could not fit through her pelvis. This is called a cephalopelvic disproportion diagnosis.
As a mom who delivered a ten pound baby, but took four hours to push her out, I always feel heartbroken when this diagnosis is given and the standard amount of time of up to four hours to push for a first time mom isn’t honored. But, it’s not my choice at the end of the day.
In Alex’s story, we ended up having a stroke of luck. This c-section decision was made right at the morning shift change. Plus, there wasn’t room for us in the OR right at that second. I told the new oncoming nurse that Alex was tired, wanted a break, but wasn’t done pushing. She wanted another try before going back to surgery since neither her or the baby were showing any signs of distress.
How The Nurse Helped Alex
I helped Alex move to her side, had her knees stacked, and a peanut ball between her knees. This is a position that helps the tailbone move back and makes a bit more space in the pelvic outlet for the baby. As she rested here, I did a hip release massage on her top hip.
The nurse believed in Alex. She went so slowly as she took over, clearly making everything take as long as possible as she took over care of Alex. After 45 minutes though, she couldn’t putter anymore and the OR was open and waiting for us.
We asked for one more chance to push. After some negotiation, the OB begrudgingly agreed, saying it was against his best advice, but he’d allow it. Then he went to do a cervical check to see where the baby was. What did he find? No cervical check was needed! Baby was so low, we could see their head the moment Alex was in the check position!
Alex Delivers Her Healthy Baby!
Alex pushed with the next contraction and her baby’s head was born. And with the next push, her healthy baby was born.
Pushing had gone from something we were forcing, and not making progress with, to something that was hardly needed at all.
In the time that we were doing practically nothing but resting up on her side, her baby rotated and descended. All without the strain that we were previously using!! The body is so good at doing what it knows how to do! And in Alex’s case, waiting clearly prevented a surgical birth.
But I Heard ACOG Doesn’t Support Laboring Down Anymore?
If you heard that ACOG (American College of Obstetrics and Gynecology) doesn’t support laboring down anymore you would be correct.
Do you want to know a big irony – in their article about laboring down, they suggest using a doula to help reduce the c-section rate instead of laboring down.
As a doula, I find that frustrating. How do doulas lower c-section rates if we can’t advocate for practices we’ve seen work over and over again that are inspired by providers who are getting their patients the BEST outcomes?
This is one of the few places where my own opinions differ from theirs. Here’s why.
What Fueled ACOG’S Position On Laboring Down?
ACOG changed their opinion on laboring down based on a study published in 2018. But this study is next to irrelevant to laboring down. How is that possible?
The First Problem With This Study
Women who were allowed to labor down on average only waited 30 minutes before beginning to push. Plus, if a baby’s head was visible at the pelvic outlet at delivery, the family was excluded from the study.
Do you remember the definition of laboring down? Waiting 2 hours after reaching complete dilation or until babies head is visible without a cervical check. Unfortunately – all the babies that actually successfully labored down were excluded.
To me this tells me they were not actually studying laboring down. Waiting 30 minutes is very different from giving babies an ample amount of time to complete their internal rotation, and align themselves for exiting their mother’s body, so it is not surprising that the amount of time pushing was almost the same.
You will not be surprised to find that after waiting 30 minutes before pushing, there was not a large difference between pushing time for the two groups. The group that pushed right away pushed for 9 minutes more than the group that waited about 30 minutes before pushing.
But they all pushed for a long time. The group that pushed right away pushed on average 84 minutes, and the group that waited for an half hour pushed on average 75 minutes.
However, even with this short amount of time difference, women who delayed pushing were less likely to have tears and more women in the immediate pushing group had 3rd or 4th degree tears than those that waited a bit before pushing. (A win for waiting to push!)
Renee’s Birth Story
I had the privilege of being with Renee for two of her births – both of them inductions. Renee is one of those lucky moms whose inductions both went fairly quickly. She had an epidural for both. With her first, I had never heard of laboring down. She pushed the traditional way where she held her breath and bore down as hard as she could.
Since she tore during that birth, she asked me if I had any strategies to prevent tearing this time. I told her about Jessica and her experience. She did the exact same thing. After a check in her second labor revealed she was 10 cm dilated, she simply asked for more time before she began pushing. She pressed her epidural button a couple times and waited.
As the nurse was waiting, she kept moving the monitor lower and lower so it would continue to track the baby’s heart rate. This baby, unlike Ashley’s was doing pretty great, there was no worry in the room.
Suddenly, it became difficult to find the baby. The nurse couldn’t get the monitor low enough!
I helped Renee move from her side to her back. As we moved, I had to lift her leg up and over her babies head, who had begun crowning. I put her leg down, as her nurse and I both went to grab a baby who was literally coming faster than anyone could have expected. Renee ultimately did not really push at all – and she had 0 tears this time around.
But Are There Other Risks Of Waiting To Push?
This is a great question and one we should talk about. Let’s look at the risks associated with laboring down found in this study, though not others.
But here are the reasons that they didn’t find laboring down so useful, in this group of women, women who labored down
- Had higher rates of chorioamnionitis in the group that delayed pushing (this is an infection not to be taken lightly)
- Had higher rates of hemorrhaging in the group that delayed pushing (although the total blood loss was the same in both groups on average. So it is likely that fewer women who delayed pushing bled, but those that did bled a bit more, and those that pushed right away were more likely to bleed, but not to a level of hemorrhaging – or had more surgical births where the threshold for hemorrhaging is a higher blood loss level)
When it comes to birth, there are pros and cons to everything. And these can sound pretty scary! And BE pretty scary if you experience them. So let’s talk a bit more about them.
Is There Another Possible Explanation For Why Women WIth Longer Pushing Phases Are At Increased Risk For These Complications?
There is plenty of research that shows that moms who spend longer times in labor are likely to hemorrhage or have infections. This is one of the things that made me feel resistant to trying laboring down or suggesting it to my moms in the beginning.
Plus, even as a doula, who has been to many births, it’s sometimes uncomfortable to be the one to suggest a delivery of care that differs from the way that it’s normally done.
Especially if that means potentially disagreeing with a nurse, midwife or OB. (Although often I see this method suggested and supported by nurses, midwives and OBs as well. You’d be surprised how differently care providers practice even within the same locations or group.) But, the amount of surgeries I was seeing during the pushing phase was striking, and much of the research convincing, so I started sharing the idea anyway.
As I’ve gone through many labors with moms that made informed decisions to try to labor down, I’ve never seen either of these outcomes, not that they aren’t possible.
But, as I’ve thought about why my experiences have been so different, I’ve realized that there are clear explanations for those outcomes that are possible, maybe even probable.
Possible Reasons For Hemorrhage
Even though the increased risk of hemorrhaging was the news highlight taken from this study – the blood loss was the same in the two groups. The group that delayed pushing for 30 minutes had a slightly lower -section rate than the group that pushed right away. And the definition of hemorrhaging is higher for moms with surgeries.
So it’s likely that this difference in definition of hemorrhage is the reason the average blood loss was the same but the rates of hemorrhages were different between the two groups.
So it’s hard to say if this is something relevant or not.
But, hemorrhaging in general is on the rise. And, it can be quite dangerous. And it can lead to much much longer recovery periods.
So let’s take a sidebar and talk about a much larger reason for the increase in hemorrhaging that is happening in the developed world right now.
Inductions.
A More Direct Way To Reduce Hemorrhaging
Rather than looking at what we do at the end of labor to prevent a small percentage of hemorrhages, we should consider the beginning of labor. Lamaze’s rule to let labor start on it’s own and avoid induction unless medically needed is one we should consider. Especially considering the most common reason for inductions is still ‘because a mother reached her due date’, not medical reasons.
How much does induction increase the risk of hemorrhage? Well let’s look at this
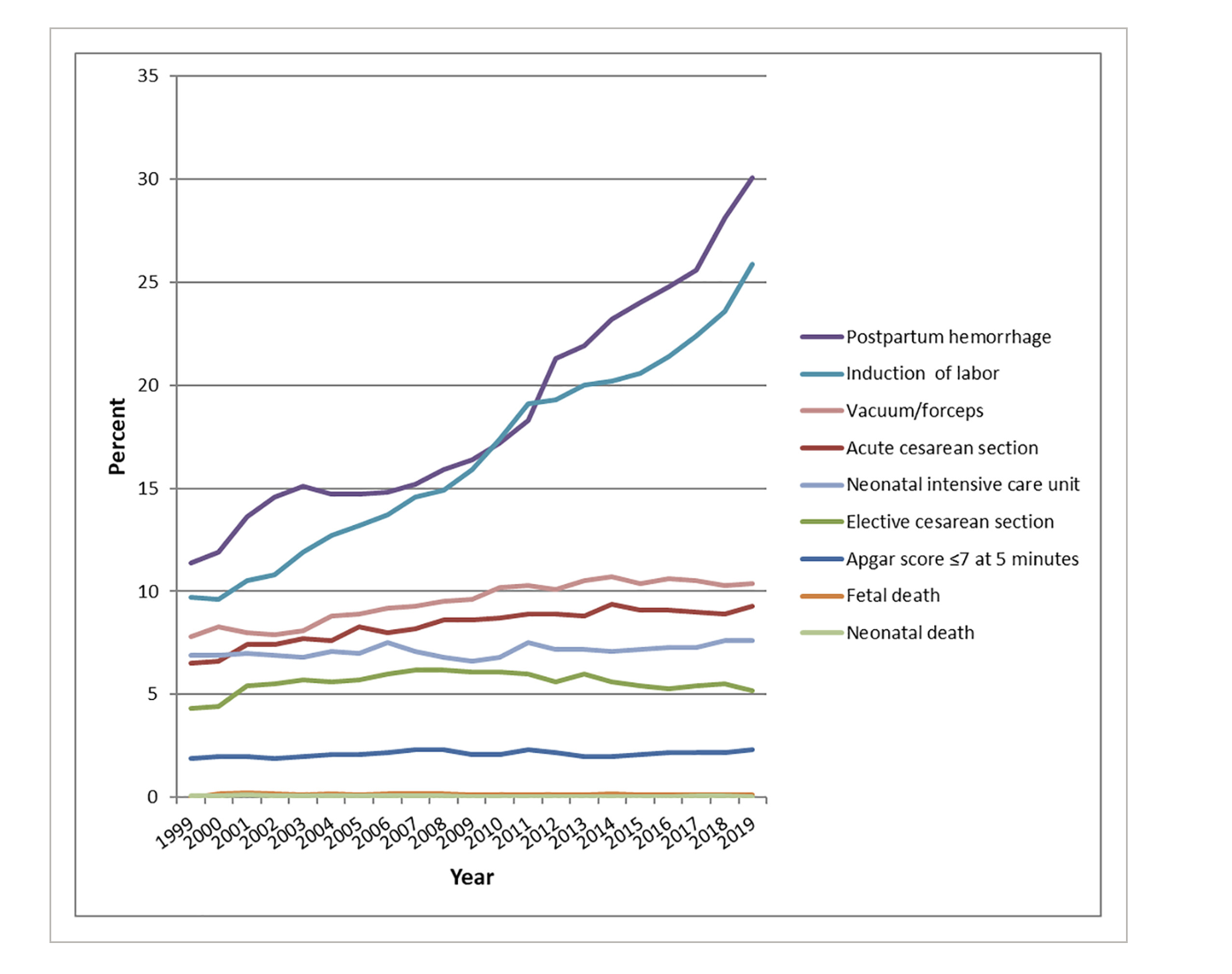
You can see that as moms are using inductions more often, the rate of hemorrhage goes up simultaneously. Probably more than most health care professionals realize.
Though hemorrhaging is a real risk of induction, I have never heard it disclosed to a mother as she is presented the option of induction. The only form of induction that has research showing it can decrease blood loss after birth is nipple stimulation. Which is a practice not supported in most hospitals.
I hope someday to be able to support more research on the subject so that it can become a more widely used practice. But, that’s for another day.
Let’s return to the risks of laboring down.
What about the Chorioamnionitis (An Infection)?
I have yet to see a case of chorioamnionitis in my moms that choose to labor down. (Though I have seen a few infections in my career in other situations and would never advocate for ignoring signs of an infection.)
But that doesn’t mean it’s not possible or more likely than if they pushed right away. But, in the 2018 study that swayed ACOGs recommendation, they did see more cases of infections in the group that waited 30 minutes before they pushed.
I have a really important question about this, that is not specified anywhere in the study. Here’s my question. In the study, they did not specify how they were giving cervical checks. Which is actually really important. One thing we know is that every single cervical check a mom has increases her risk for infections.
That makes a randomized control study like this pretty hard to do well. Why? Because what happens if you delay or minimize cervical checks? You might miss moms that labored down or in this case, exclude them from the study all together.
This makes sense, because in a randomized control study, people stay in the groups they were put in. So if a mom did labor down, but was in the don’t labor down group, her result would still be counted as a ‘did not labor down’ even though she did labor down. (I know – confusing.)
Which in fact did happen. In this study, in all cases where the fetal head was visible at the introitus at complete cervical dilation their data was excluded. If you go back to our definition of laboring down, this is the exact situation we are trying to create.
Infection Risks Continued
In fact, out of the more than 12,000 women that were originally included in the study, nearly 10,000 of them were excluded. For this, and other reasons, which we will talk about later.
As a doula that’s attended 200+ births, I have only seen this situation where the baby’s head is visible at the entrance of the vagina when a mother was given time to labor down. Either a patient asked to labor down, or a nurse advised a patient to delay cervical checks so she could labor down.
Clearly, some moms were allowed to labor down because the care team didn’t do enough cervical checks to identify when they reached 10 cm dilated. This is often a purposeful decision at the end of labor. Truthfully, I want to give all these providers a high five for excellent care.
They limited the risk of chorioamnionitis by not doing excessive cervical checks and allowed babies to come down before pushing. This should be the gold standard of care! Instead, this combo of limited checks and laboring down was excluded from the study.
Many times in labor, being hands off, but attentive is the best way to support a woman and baby!
But, if you don’t want to miss reaching 10 cm? What do you do? More cervical checks. And what is that going to result in? More cases of infection. Which did happen in the mothers who were not excluded from the study.
So What Do We Know From This Policy Changing Study?
While this study changed ACOG’s view of laboring down, I think we need to have a critical eye about it.
One, it doesn’t actually clearly define laboring down and the only mothers that actually labored down were excluded from the study results.
Two, its findings are not in line with other research that has shown clear benefits and safety of laboring down.
Three, it does not have any discussion of how they control for other factors that could increase hemorrhage or chorioamnionitis. Which, they likely could have caused by the other moving factors in the labor and care process.
Birth is not easy, and I don’t envy you in having to make your choices about laboring down. All I can say is that for my moms that have labored down, I’ve seen much happier moms.
Madura’s Birth Story
Madura was a mom I worked with who was having her first baby. We had talked about laboring down, but she didn’t know what she wanted to do. She was ultimately leaving it up to the provider on call that day.
As her labor progressed, just like Jessica and Renee, Madura began feeling pressure in her bottom, even with her epidural. She pressed her epidural button to get a bit more pain relief and when she started telling me she felt like she had to poop, we told her nurse.
Her nurse smiled too. You could see she was excited. The nurse checked the clock, and let Madura know that she was due for another cervical check. But, that we also had the option of waiting until the midwife came back, who was scheduled to drop by in 2 hours.
Then she told Madura, if I check you now and you are complete, we will start pushing. But, it is in your best interest to wait and see what happens when the midwife gets here.
When the midwife came in a couple hours later, Madura was not just fully dilated, but her baby was just about ready to be born.
This is the mom I mentioned earlier that pushed for a grand total of 9 minutes.
Her nurse purposefully suggested and allowed her time to labor down, without us even needing to ask for it! And, she helped prevent the risk of infections by not doing cervical checks that weren’t necessarily needed. I wish I always got to work with this nurse!!!
Why Is Getting Quality Information About Best Practices In Labor So Hard?
At the beginning of this article, we talked about a midwifery group where 99% of moms had either a first degree tear or no tear at all. If we know this is possible, why isn’t it happening everywhere? Well, medical systems and medical training are complicated.
Can you imagine you’re sitting in an advanced calculus class and the teacher says, raise your hand if you got an A on the last test? Now put them down. Now raise your hand if you got a B? Ok. Great. Now Cs? Okay who got a D? And who is flat out Failing?
Then can you imagine if the next thing they said was alright, if your hand is up and you got a D, or an F, you will be teaching the rest of this class!
This is exactly what is happening in the birth world. Unfortunately, the majority of studies, this one being a great example, are published by hospitals providing unacceptably poor care.
What Do I Mean By That?
The World Health Organization (WHO) has long claimed that the optimal cesarean rate is between 5 and 10 percent of births, and that any rate above 15 percent is doing more harm than good. And there are plenty of hospitals that meet that criteria for ALL of their moms (not just a very select group of low risk moms as is in this study).
So from there, we can conclude, hospitals that have c-section rates between 0-10% – celebrate them as A students. 11-20%, they are doing pretty good, we give them a B. 20-30% hmm – they need a tutor from one of the other hospitals to come help out, because C’s are not so good. A hospital with a c-section rate of 30%-40%, our D students. They really are struggling.
Unfortunately, not all the hospitals report their c-section rates. But many do. How are the hospitals in this study doing?
3 of the 5 of them have c-section rates above 30%. U Penn, is crazy close at 29% and Oregon is doing pretty good, with a 21% NVST (first time low risk c-section rate. )
C-Section Rates For Hospital In This Study:
Washington University in St. Louis School of Medicine; unreported
University Of Alabama Birmingham – 38% c-section rate in 2020
Oregon Health and Sciences University reports: Our NTSV (Nulliparous, Term, Singleton, Vertex) cesarean birth rate is 21%. This means that 21% for first time, low risk head down babies.
University of Pennsylvania 29% .
Missouri Baptist Medical Center – more than 30% NVST rate (first time, low risk moms + babies, and head down)
Pennsylvania Hospital 30%
Why Does This Matter?
When we are looking at the value of research, we need to consider more than if they followed the process of a Randomized Control Trial or not. We need to consider the results they are getting for their moms.
Just like in math, if you make a mistake early on in labor, it might not really matter what you do later down the road, you’re still going to end up at a different outcome than you wanted.
In this study, the one that changed ACOGs perspective on laboring down, the study that is being used to define the ‘best practice’ of medicine, the c-section rates for the two, nearly identical groups were 15% (the group that waited 30 minutes to push) and 16% (the group that pushed right away) respectively.
Now, consider, these are the healthiest moms, at term, no twins or other multiples, no moms with health conditions like preeclampsia, or gestational diabetes, no breech babies, or moms with placenta previa where surgery absolutely makes sense right from the beginning. If babies had any fetal distress before pushing they were excluded and taken out of the study.
So, after taking out ALL the moms that had risk factors of any kind, and removing all the babies that showed any signs of not tolerating the birth process, and after getting all the way through 95% of the labor process, they still are nearly 2 times the acceptable c-section rate for all moms.
Does That Concern You?
The only thing this study should conclude is that these hospitals need help. They should not be guiding the rest of the country in best practices of care for moms. They need to go back to the drawing board and learn from hospitals that are getting better results.
In fact, there are hospitals where the c-section rate is only 7%, and that includes their high risk moms, their multiples, their breech babies, their moms with placenta previa, EVERYONE.
Evidence based birth would be much easier to understand if ONLY these hospitals that are our A students, whose actual outcomes for all of their mothers, were allowed to publish their results or guide policy. It would be much clearer what actually works and what does not.
I wish the conclusion drawn from this study was a plea for help, not an expectation of respect and admiration because they could go through the process of publishing research, even if the results are SO POOR they should mean nothing.
How Did My Results Change After Laboring Down?
If you remember the start of this story, my interest in laboring down developed because I was having too many moms going back for surgeries in the pushing phase of labor. (yes, here in Seattle, many of our hospitals have 30%+ c-section rates, so self advocacy here is important)

These are the NVST (first time, at term, head down babies) c-section rates for our local hospitals. from Jan-Jun 2022, the latest information available at the time I made the reel.
Well, last year, 2023, I only had 2 moms go back for surgery during the pushing phase of labor. My most common reason for a surgical birth? No longer long labors and epidurals. Now, it’s Breech babies. And I’m excited to learn more about how to help these little ones flip before labor.
But, what happened in those two labors where moms had surgical births after making it all the way to the pushing stage?
In the first one, I suggested laboring down and was told flat out ‘no, we don’t do that here.’ Her story was just like Alex’s, but without the change of shift that gave us extra time.
In the second one, when I suggested laboring down with a mom whose baby was at 0 station, the OB said, ‘great, I love that idea, I’ll be back in 15 minutes.’ When I tried to clarify and define laboring down for him, he disagreed. We started pushing 15 minutes later.
After 2 hours of pushing, he called for a surgery because the baby was ‘in a bad position and wasn’t going to fit’.
Does it feel like you’ve heard that before?
What Has Success With Laboring Down Looked Like?
In the past year, I have had many moms ‘push’ for less than 15 minutes. I have had many epidural moms have 0 tears. I even caught my first baby because an OB wasn’t quite fast enough getting into the room and gearing up. (Ooops – that was not intentional!)
I am starting to feel that pushing for very short amounts of time and not tearing are not only possible, but probable when care is approached in this way.
So maybe my data is not that significant. This is not a randomized control study. My cohort is small.
But, I am proud of the results I’ve gotten for my moms and hope to help more moms trust in their own body. I also hope that as moms read this, they will gain confidence in speaking up and asking for more time if they are feeling rushed or pushed through the pushing part of labor.
With every success, my voice grows louder, as does my ability to communicate and collaborate with the teams I work with at the hospital. I hope reading this helped your voice grow as well.
Is Laboring Down Ever Not Appropriate?
Of course, laboring down will not solve every problem. Birth is complicated. If a baby is in distress and needs immediate help, then that should be addressed in the best way possible under the direction of your skilled provider. Infections and distress should not be ignored in the name of laboring down.
What If I Just Want To Try Pushing Right At 10 CM?
I’d also like to share the story of Christine with you. Christine wanted a natural labor, but as she neared the end of her pregnancy, an induction became necessary. With the Pitocin, the contractions became too strong to handle and she opted for an epidural.
Even though her baby was high when she started pushing, she pushed right away and had her baby in 45 minutes. Some babies are just ready to be born. And some moms push and move their babies right away!
In fact, she did not need direction at all! She did this all on her own. So if you’re 10 cm and you want to start trying, go for it. Maybe this will be you.
I hope this article helps you advocate for more time if you and baby are well but you are running up against a clock of any kind. Sometimes, all moms need is more time.
For my moms that prefer immediate pushing, I am in 100% support of that and am behind them all the way. My job as a doula is to make sure you have access to information and then help you implement the plan YOU decide.
Are There Any Alternatives To Delayed Pushing Or Immediate Pushing?
You know what, if all this feels overwhelming, it’s okay. The goal here is to give you ideas, knowledge and opportunities to advocate for yourself. If you do start pushing at 10 cm and move your baby quickly! That’s amazing.
If you do start pushing at 10 cm and your baby seems like they aren’t moving, now you know you can ask (or demand) a break and a period of waiting before you move on. And that you should say no to cervical checks in this time.
There’s also a third option. Usually, when moms are pushing with an epidural, they are told to hold their breath and push hard for 10 seconds. A new study shows that a more optimal pushing time is only 5 seconds of pushing with each push.
This study also clearly states that active pushing time is a more relevant measurement for risks of the pushing stage than total duration of the third stage of labor. Which further supports the idea of laboring down.
However, I do not have any stories with this method of pushing with shorter increments because the only times I’ve suggested it I’ve been told “that’s not how we do things here.”
I think you will find that as your labor unfolds, you will find it easy and natural to know what you need at this stage. Tune in with your body. You will know what to do! Your intuition will lead you and you will make the right choices for YOU.
Laboring Down TL/DR
I cannot promise that laboring down will help every mom prevent tearing, forceps, episiotomies and surgical births. But I can say this. Since introducing laboring down into my practice, it does not surprise me when moms with epidurals push 5, 10 or 15 minutes total. I often (but not always) see 0 tears when pushing with an epidural.
I also see a lot of resistance to the idea from some care providers and other care providers that love it.
I hope you have a great experience with your birth and that this information helps you make decisions around pushing that work well for you.
Congratulations mama!
