
- Five Best Iron-Rich Snacks For Pregnant Moms To Avoid An Iron Deficiency - February 26, 2026
- Eat These Five Meals On Repeat For The Best Sources Of Iron In Pregnancy - February 19, 2026
- 5 Surprising Signs Of Iron Deficiency In Pregnancy - February 12, 2026
Your hands rest on your belly, you feel your baby kick. As you lay in bed, you can imagine your life with this perfect new little person you made. But, thinking about the process of bringing them here is filling you with anxiety. Though you’d like to deny it, you’re worrying about the birth process.
You looked up your hospital’s c-section rate and were surprised by how high it is. You hope everything goes smoothly. It seems smart to avoid interventions.
But on the other hand, what if you need them? How can you know if you the suggestions made by your care team are in your best interest or a matter of convenience?
If this worry has kept you up at night, you are not alone. My name is Suzzie, and I have been a doula for five years. I cannot tell you the number of times mother’s come to me with worries about unnecessary c-sections. Like you, they want to make the right choices for themselves and for their baby.
By the time you finish reading this article, you will understand why reducing unnecessary c-sections is so important, how one hospital cut their c-section rate in half, and 4 simple things you can ask for to help you avoid an unnecessary c-section in your birth, while also having confidence that if a surgical birth is right for you, you will get the help you need.
Are you ready? Let’s do it!
Why Is Reducing The C-Section Rate Important In The First Place?
When it comes to surgical births vs going through labor and having a physiological birth, there is a lot to consider. On one hand, a surgical birth is a very quick procedure. One that can save the life of a mother or a child when used in the right situation.
On the other hand, surgical births come with quite a few downsides, some of them bigger than you might think.
On top of that, women today are 500 times more likely to have a c-section than women in the 1970s when the c-section rate was only 5.5% (Shah).
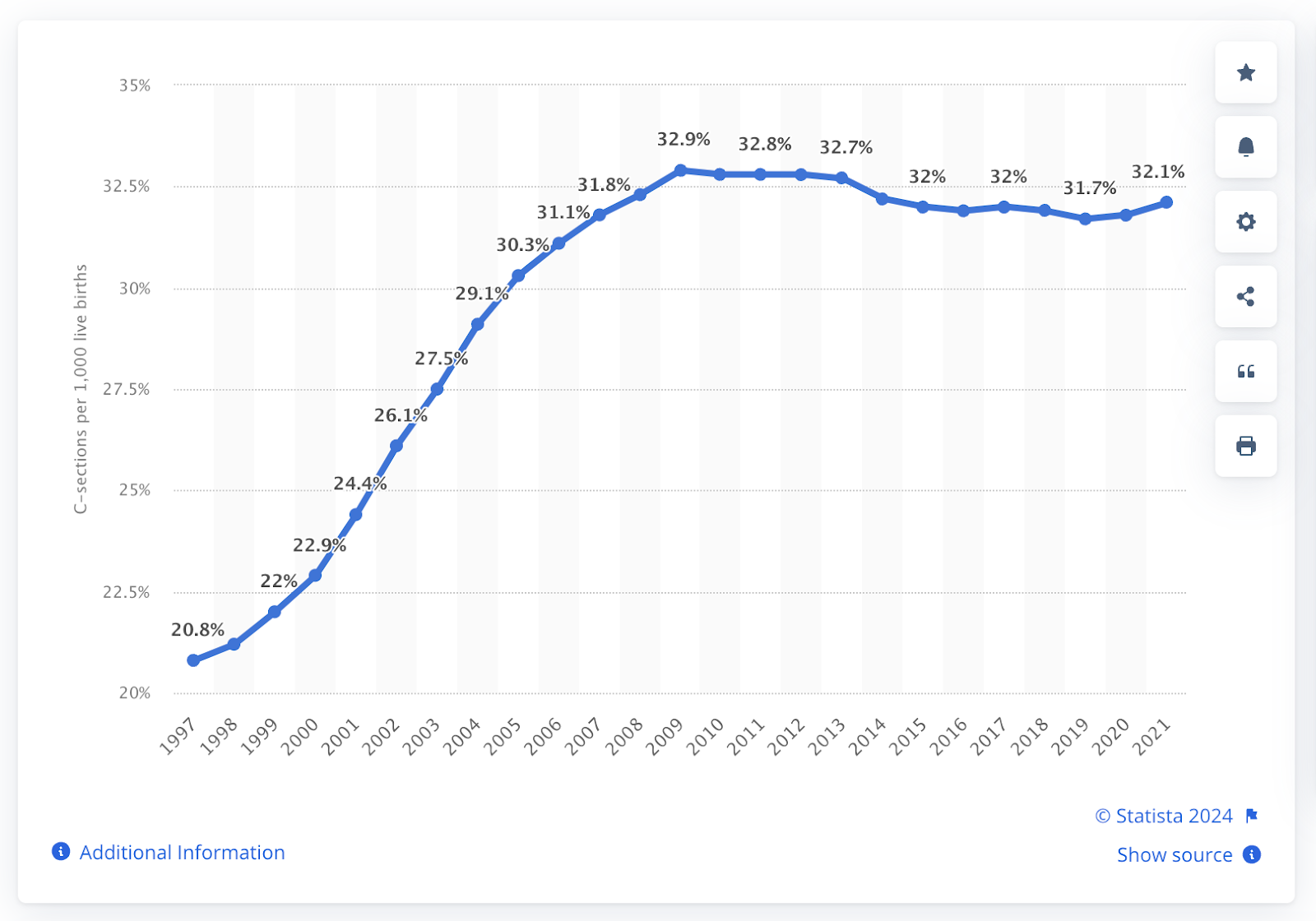
Though this chart does not go back all the way to the 1970s, you can see how sharp the rise was before we plateaued at 1 in 3 mothers giving birth by surgery.
What Are The Downsides Of Surgical Births?
Of course, if giving birth by surgery saves a life, all other downsides seem unimportant. But, if surgical births can have such a huge positive impact, why doesn’t everyone opt for surgical birth? Well, the truth is that the pros and cons of a surgical birth shift depending on a mother’s and baby’s personal health situation.
Surgical births in general, carry much greater risk to both a mother and a baby than going through the labor process, except in very specific cases when a mother or child can no longer tolerate labor.
So what are the downsides of a c-section? Even after controlling for risk factors that might have made a C-section more likely, the risk of death after the procedure is 3.6 times higher than after a vaginal birth.
The most common complications that could lead to a loss of a mother from a surgical birth are complications from the anesthesia, puerperal infection and venous thromboembolism.
(On the other more reassuring hand, if a surgical birth plan is in your story, keep in mind that 99,987 out of 100,000 times, moms will be going home with their baby a few days after surgery. That’s 99.987% of the time.)
What Are The Other Downsides Of A Surgical Birth?
C-sections have additional risks as well. Other complications such as hemorrhage, infection and organ injury are three times more likely to occur with a cesarean compared with a vaginal delivery – risks that increase with each subsequent surgical birth a mother has.
Even in the absence of complications, taking care of a newborn infant is a much more difficult task when a mother has a 10-centimeter incision on her abdomen. (source)
Not to mention that if you are wanting more children after your surgery, every future birth you have after your first surgical birth will now be riskier than it would have been without a surgical birth.
In future pregnancies, moms who have had a previous surgical birth are more likely to have placental problems such as previa, abruption and accreta – all of which can be quite dangerous on their own. Risks rise with each repeated c-section. (source)
Most surgical births go quite well, so these risks are often overlooked and very rarely discussed because by the time surgery is suggested, it is usually the best option, even with all the extra risks.
How Common Are Unnecessary C-Sections?
The World Health Organization (WHO) has long claimed that the optimal cesarean rate is between 5 and 10 percent of births, and that any rate above 15 percent is likely to do more harm than good (Wolf).
Currently, over 30% of moms give birth by surgery. Meaning the amount of moms having surgery is more than double the acceptable rate. Half of all c-section are unnecessary, or could have been prevented with different care.
Can A Hospital With A High C-Section Rate Reduce Unnecessary C-Sections Without Endangering Mothers Or Babies?
Here is the golden question, one that many people who work with pregnant and expecting mothers are asking. The good news is, we now have definitive proof.
Recently, a Colorado community hospital recognized that it’s c-section rate of 28.9% was too high. They set out on a 12 month improvement project to bring it down. And with only four simple changes, they brought their c-section rate down to only 12.2%.
So what did they do?
- Reduced elective induction of labor in women less than 41 weeks’ gestation
- Standardized triage to admit women at greater than or equal to 4 cm dilation
- Increased the use of intermittent auscultation as opposed to continuous fetal monitoring for fetal surveillance
- The team also calculated each obstetrician-gynecologist’s primary cesarean birth rate monthly and delivered these rates to the providers.
The great thing about these changes are that they are not complicated, there is a lot of evidence behind each practice, and, as a mom, these are things you can be proactive about in your own birth as well.
Should we take a deeper look at each of these practices?
Reducing Unnecessary C-Sections Practice 1: Avoid Elective Inductions Before 41 Weeks
Inductions, or forcing labor to start instead of waiting for the body to go into labor on it’s own, is one of the most common interventions being offered to mothers today.
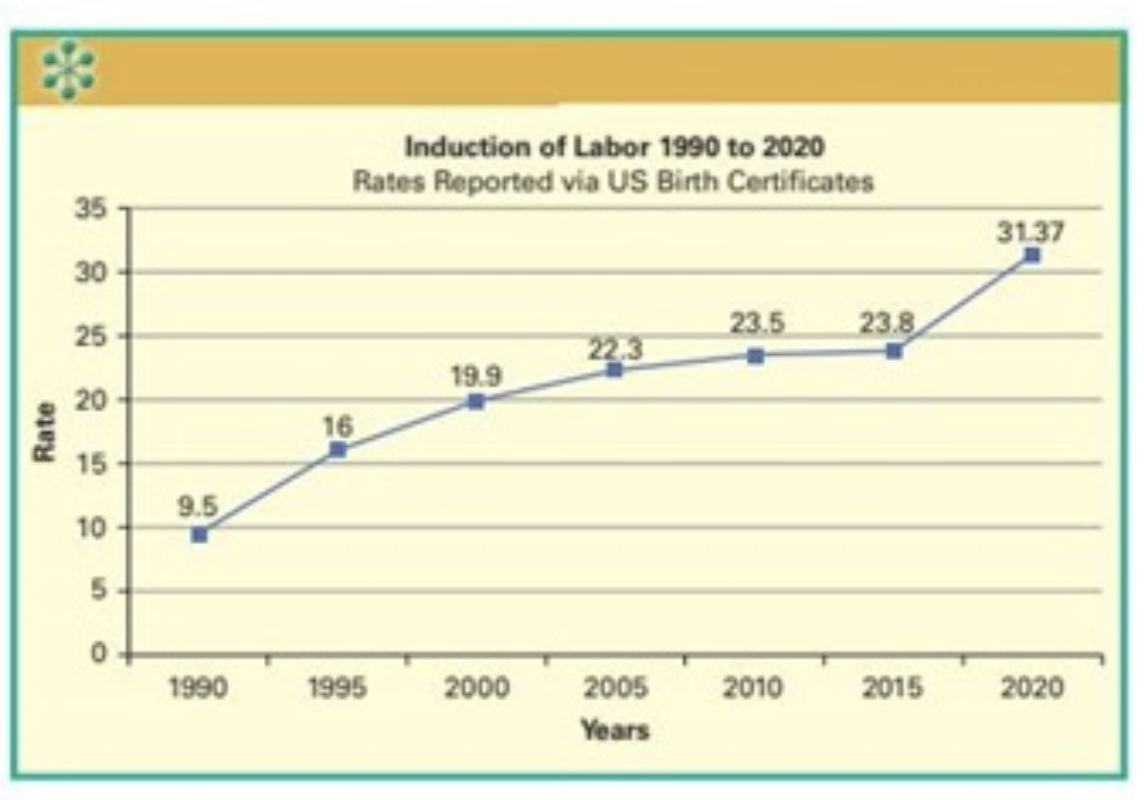
In the 90s, only 10% of births were induced, now over 1 in 3 moms will have their labor started via a medical route. Too often, just because we can. (link)
The listening mother’s survey in California found that the most common reason doctors suggest inductions is not because of a medical problem, but simply because a mom has reached or is nearing her due date.
Can Early Inductions At 38 Weeks Prevent Surgical Births?
In 2018 a landmark study was published in the Journal Of Obstetrics and Gynecology. It is called the ARRIVE trial.
Basically, they were looking to see if they could reduce the c-section rate by inducing at 39 weeks instead of waiting for labor to start on it’s own. Historically, although babies are considered full term at 40 weeks, labor was not induced until 42 weeks. By this time, most moms will have entered labor on their own.
You may be surprised to hear me say that they were successful in reducing c-section by inducing at 39 weeks! Yes, a full week before a mother is considered full term.
But by how much? 22% of moms who waited for labor to start on it’s own had a surgical birth, compared to 19% who started with an induction. The reduction in surgical births was 3%!
But, are you noticing something a bit funny about this research? Doesn’t 19% still seem high to you? It does to me.
Especially considering that these were all low risk moms. There were no moms with gestational diabetes, no moms with preeclampsia, there was no fetal distress prior to labor, no babies born before they were term.
Essentially, they had the healthiest of healthy moms all at term and with head down babies.
They excluded every mom and baby who started the labor process with a likelihood of a needed an surgical birth, and they still missed the mark of a 5-15% c-section rate.
In my opinion, this makes this study invalid. It’s finding should not be applied to clinical practice. However, I hear many of my moms being told ‘if you induce early you will have a lower chance for a c-section.’ My observation is this is not true and data would support that opinion.
What Happened After The ARRIVE Trial?
The ARRIVE trial was published several years ago, and induction by choice has increased significantly.
One hospital, with a historically low c-section rate looked at what happened in their hospital after the publication of the ARRIVE trial and the popularization of induction at 39 weeks.
Their results tell a much different story.
The rate of cesarean delivery among electively induced women increased from 6.5% to 14.8% in this group of electively induced women.
Their induced moms also had longer hospital stays, increased blood loss, and lower birth weights.
The increased likelihood of a surgical birth following a medical induction has been found in multiple studies.
Including this one, which found surgical birth rates went up from 10% to 19% from the group that did not attempt to induce labor, compared to the group that did induce labor.
The point of this being that just because a study is published, doesn’t make the result of that study a best practice for all moms to follow.
In the absence of an actual medical problem, it is best to let labor start on it’s own.
So, if you are told to electively induce at 39 weeks of pregnancy without a medical reason, or your provider mentions the ARRIVE trial, it’s okay to give push back. The ARRIVE trial did not set a new evidence based best practice. And inducing early does not seem to reduce unnecessary c-sections in actual practice.
Reducing Unnecessary C-Sections Practice 2: Stay At Home Until Labor Is Well Established
Okay, so you now know how to apply the first rule. Wait until at least 41 weeks to induce in the absence of a medical reason. Let’s talk about the next thing you can do to reduce unnecessary c-sections: wait to go to the hospital until labor is well established.
Have you ever heard a story of a mom heading to the hospital, getting to triage, and being told to walk around and come back? This may seem counter-intuitive for many. Aren’t you supposed to rush to the hospital at the first sign of a contraction?
Well, it does make sense to call and open a line of communication, especially if something feels off. ALWAYS address anything that seems off to you.
But, in most cases, it makes sense to stay at home until labor is well established.
In my area, most hospitals suggest coming in when contractions are between 4-5 minutes apart, are a minute long and have been that way for an hour.
Typically, moms are just entering active labor at this point. And waiting to head in until labor is established absolutely lowers your chance of a surgical birth. Check this out:

According to the listening Mother’s Survey, moms, who arrive to the hospital at 4 centimeters or more dilated, are much less likely to have a surgical birth than those that rush to the hospital.
So practice your labor coping skills, learn to time contractions, and when labor starts, wait until you hit that 5-1-1 rule to head in.
Not sure what you will do in this time? Check out our childbirth class to learn all the skills you need to handle contractions like a boss!
Reducing Unnecessary C-Sections Practice 3: Ask For Intermittent Monitoring Instead Of Using The Continuous Monitoring Option
To recap, you now have 2 things to do to reduce the risk of an unnecessary c-section. First, waiting until 41 weeks to induce or wait for labor to start on it’s own. Second, wait to go into the hospital until labor is well established.
Now let’s talk about the next option. How your baby is monitored during labor.
As of the time I am writing this, the most common way to monitor the health and safety of a baby is continuous monitoring. But we have decades of research that shows that intermittent monitoring is actually the better practice for low risk moms and babies.
What Is Intermittent Monitoring?
When you are monitored intermittently, instead of a machine being strapped to you to listen to your baby all the time, a nurse comes in at regular intervals and uses a doppler to listen to the baby’s heart rate personally.
I’m not going to lie. This option feels a bit scary to many moms, because it’s a bit counterintuitive. In most hospitals, the moment you get checked in, a baby monitor will be strapped to your belly so you can hear your baby’s heart rate 100% of the time.
It seems like this would make birth safer for the baby. After all, knowing exactly what is happening at every moment should help a care team intervene and support a struggling baby earlier. (And it is very important during inductions when you are using strong medicines like misoprostol and pitocin that even when used correctly can put excess strain on a baby.)
But, actually, continual monitoring in a labor that started on it’s own, has been shown to do more harm than good.
That is why many organizations that recommend best practices discourage the routine use of continuous monitoring during labor, including: the Society of Obstetrics and Gynecologists of Canada; National Institute for Health and Care Excellence in the U.K.; American College of Nurse Midwives and the California Maternal Quality Care Collaborative in the U.S.
Why Could Intermittent Monitoring Be Better?
As a doula, I do not have all the answers, and the research on intermittent monitoring doesn’t necessarily say why it is safer, just that it is safer. But, this is my observation.
Intermittent monitoring requires more actual attention on you than continuous, which requires attention to the machines watching you, not you. A nurse who has to stand close to you and listen to your belly is going to notice when your lips are dry and can recommend you drink a sip of water before your dehydration becomes a problem.
She is likely to see you working through contractions, and offer more encouragement, especially if her training in monitoring encouraged her to interrupt you as little as possible as she does it.
She is likely to encourage you to walk, and move, and use other tools to cope with labor, because she is intrinsically more involved in the labor process and closer to you through labor.
When we use only continuous monitoring, care teams can be so focused on the strip that they are not proactive with the little things in your labor until they become big things, and much more difficult to deal with.
Reducing Unnecessary C-Sections Practice 4: Ask About Your Doctor’s C-Section Rate
When it comes to reducing unnecessary c-sections, simply knowing your doctors or hospitals c-section rate is important. Why? Because in a relationship where you are literally putting your life in someone else’s hands, it’s important to know the results they get.
Trust must be earned when it comes to the sacred doctor/midwife relationship with their patients. And the path to earning your trust, the trust of the mother, is in having great results.
Your doctor may not know their c-section rates. But, by looking up your hospitals rate, you may get a good sense.
You will also know if your doctor even cares about reducing unnecessary c-sections from the way they answer the questions. Are they thoughtful? Do they have reasons why their rate is high? Are they working on specific things to bring it down? Or do they already have that 15% or less c-section rate.
When it comes time to make decisions in your birth, this will help you be able to build a trusting relationship with your provider.
I always teach my clients that trust is built on authenticity, empathy, logic and followthrough. If your conversations are based on these things, you can bet you are receiving good advice and are not heading to an unnecessary c-section, even if you do ultimately have a surgical birth.
Reducing Unnecessary C-Sections TL/DR
It is true that in the United States, and many other developed nations, the number of mother’s giving birth by c-section is much higher than reasonable. So, if you are hoping to avoid an unnecessary c-section, it is good to prepare and take simple steps to reduce your risks.
There are 4 evidence based practices that you can ask for in your labor.
- Delay any elective inductions to 41 weeks.
- Stay at home until labor is well established.
- Choose intermittent monitoring instead of continuous monitoring.
- Know you doctor’s (or hospital’s) c-section rate and have thoughtful conversations about it.
If you follow these tips, you will reduce your risk for a surgical birth. Now, as a doula and childbirth educator, I would love to help you prepare for labor. Inside my childbirth course you will find everything you need to be able to cope with labor with confidence. And guess what? Studies show that taking a childbirth class reduces your c-section rate as well!
Here’s to you having a safe and healthy birthing experience!
